Third Party Order Form (print and include with cheque)
| Date: {date_mdy}To: RSRS – Record Storage & Retrieval Services Inc. 111 St. Regis Cres. S. Toronto, ON M3J 1Y6 |
From: |
| For: Retrieval of Medical Record From the medical practice of Dr. {Doctor’s First Name:1} {Doctor’s Last Name:2} in {Doctor’s City:3}, {Doctor’s Province:4}. Medical Record of {Patient First Name:5} {Patient Last Name:6} D.O.B.: {Patient Date of Birth:7} Date Last Seen: {Date patient was last seen by doctor, (if known):8} {or choose an estimated date range when patient was last seen by doctor (choose only one):9} |
|
| Service |
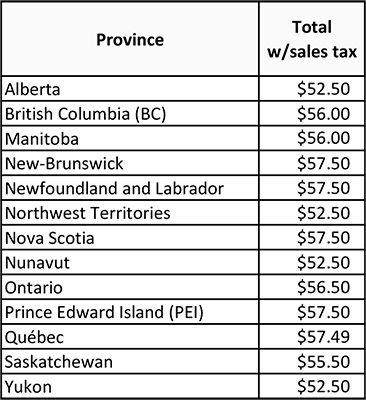
| Initial Medical Record Search
Look-up your province and find the total cost of the initial search fee, including sales tax, in the right column: |
| Special Requests: {Comments:29} |
|
Remember to include: [ ] This order form (print) [ ] Release of information, signed by patient (or legally authorized representative) [ ] Cheque for $50.00 plus sales tax made payable to “RSRS Inc.” |
|
Please note:
|
Thanks you for your order. We will get in touch with you shortly.